
Women and COVID-19 Vaccine in
East and Southern Africa
A Data Snapshot on Vaccine Demand and Access among women in ESAR – August 2022
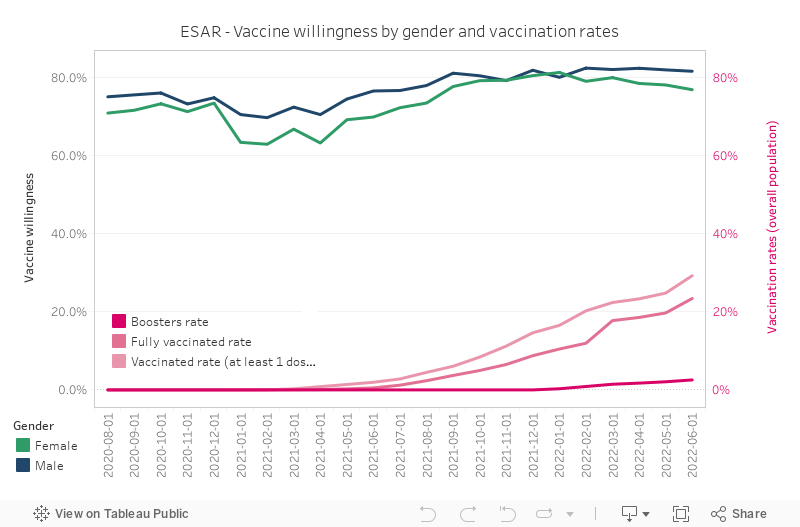
As of September 2022, over 235 million people have received their primary (initial) series of a COVID-19 vaccine in Africa. This figure represents 20% of the African population. There are also significant differences between vaccine willingness and vaccine uptake within the two African regions – West and Central African Region (WCAR), East and Southern African Region (ESAR) – from which the Collective Service COVID-19 Behavioural Dashboard routinely collects data. For example, in ESAR, 79.5% of the population state they are willing to be vaccinated if a vaccine is available (which is a comparable figure to the European Regions’ 83% vaccine willingness). However, only 25% of the ESAR population has received two doses of a COVID-19 vaccine.
The pandemic has also exacerbated the gender gap. As stated by UN Women: “The brunt of the pandemic has been borne by women and girls.” Globally, women’s access to health services was interrupted (including sexual and reproductive health care services), their access to digital technologies reduced (impacting access to timely information), and their mental and emotional well-being strained (often as a result of increased domestic responsibilities paired with decreased access to basic goods and services). For example, more women than men in five[1] out of the six countries UN Women surveyed in ESAR, reported that their psychological, mental or emotional health was affected by the pandemic.
Beyond the notable geographic disparity between willingness and uptake in the ESAR region (among all populations), a gender gap is evident with women’s intention to be vaccinated lower than men’s. What data is available to help understand the growing gap between willingness and uptake among women in the region?
[1] Eswatini, Ethiopia, Kenya, Mozambique and South Africa.
As elaborated by Butler et al. in a recent study conducted on increasing vaccination rates amongst South Sudanese women, COVID-19 vaccine uptake is based on several psychological (vaccine confidence, risk perception, knowledge and awareness), social (gender norms and power relations, cultural and religious beliefs, social influences) and practical (vaccine roll-out challenges, access, time constraints, (in)security, access to information) considerations. This data snapshot takes a deeper look into potential reasons for vaccine hesitancy among ESAR women, as well as highlighting some specific access related issues they face.
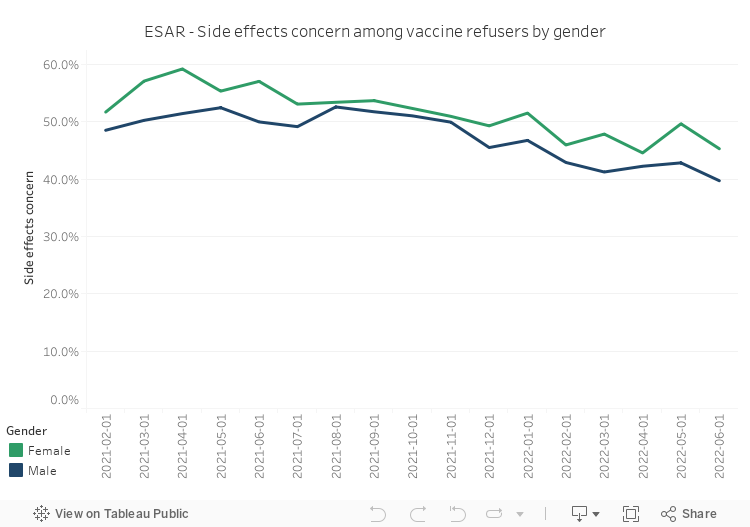
Women in sub-Saharan Africa are more likely to report concerns over side effects (in general) as a reason to explain their vaccine-related hesitancy or refusal. Behavioural Dashboard data from ESAR illustrating increased concerns among women, supports this finding (see chart below). The spread of misinformation on side effects, specifically for pregnant women, is a known and ongoing challenge in the region raising fears and concerns, perhaps particularly amongst women of child-bearing age (VOA, 2021).
“According to Phionah Atuhebwe, MBBS, MPH, the new vaccines introduction officer of the World Health Organization’s Regional Office for Africa, online rumors about vaccine effects on fertility and pregnancy have regularly appeared since the vaccine rollout started, particularly during its early phases.” (Feb. 2022)
We know that women have fared better in countries with targeted social protection policies aimed at mitigating the disproportionate impact the pandemic has had upon them (UN Women, 2021). In the absence of consistent national guidance targeting specific COVID-19 informational and health service concerns of women and families, their needs may have been ignored or overlooked.
“… Low vaccine acceptance among women, especially pregnant and breastfeeding, may be due to a lack of firm and consistent guidance in national policy regarding COVID-19 vaccination.” (Apr. 2022)
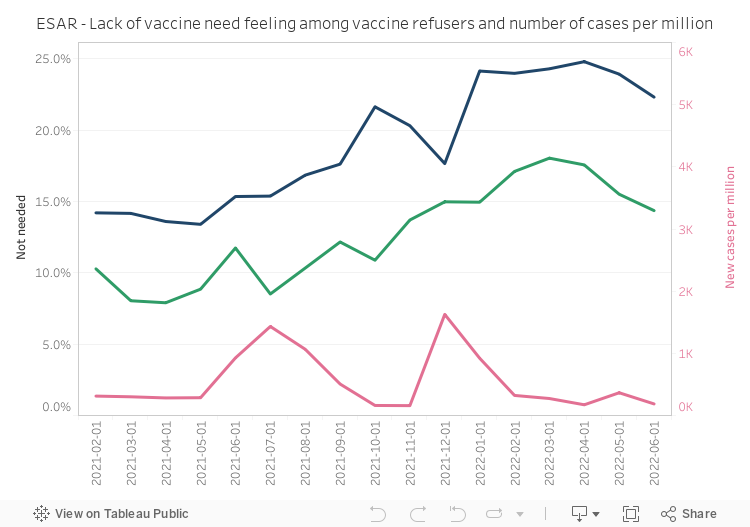
Quantitative data from the Behavioural Dashboard also highlights that women in ESAR are far less likely than men to explain their vaccine-related hesitancy or refusal due to a lack of need.
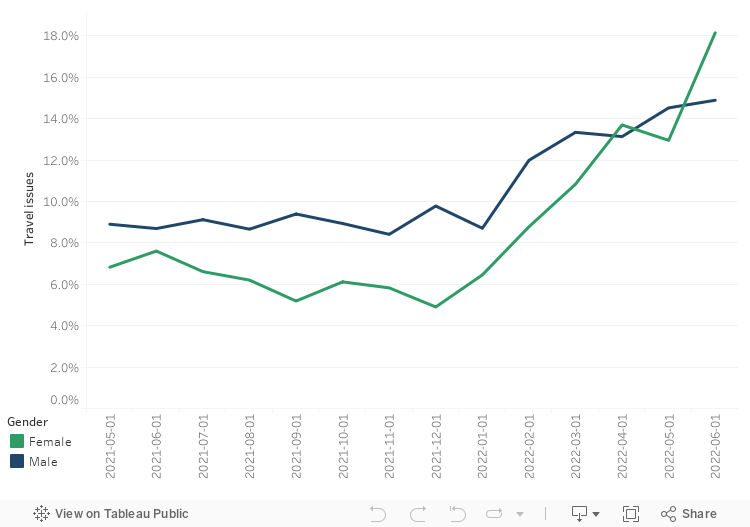
Access-related issues
COVID-19 vaccine campaigns in Africa have increased with greater access to the global supply chain, however, access-related travel (cost, distance) and health-facility (no appointment, hours of operation) issues remain a barrier to vaccine uptake. For example, among women in ESAR (especially within the last few months), there has been a sharp uptick in reported travel issues. UN Women has also found that slightly more women than men, in both ESAR and WCAR, reported access to medical care is more difficult since the pandemic began.
- UN Women – Women and girls left behind: Glaring gaps in pandemic responses
- Oxfam – 5 ways women and girls have been the hardest hit by Covid-19
- Butler N. et al. (2022) – Key Considerations: Improving Uptake of the COVID-19 Vaccine Amongst Women in South Sudan
- Abassi J. (2022) – Widespread Misinformation About Infertility Continues to Create COVID-19 Vaccine Hesitancy
- Taye et al. (2022) – COVID-19 vaccine acceptance and associated factors among women attending antenatal and postnatal cares in Central Gondar Zone public hospitals, Northwest Ethiopia
- Adeyanju G. et al. (2021) – Examining Enablers of Vaccine Hesitancy Toward Routine Childhood and Adolescent Vaccination in Malawi
- Sethy G. et al. (2022) – A Retrospective Analysis of the COVID-19 Vaccine Express Strategy in Malawi: An Effort to Reach the Un-Reach
- Ackah B. et al. (2022) – COVID-19 vaccine hesitancy in Africa: a scoping review
- WHO Afro – Africa COVID-19 Vaccination Dashboard (accessed on 2022-09-06).
- Collective Service – Global Social Behavioural Dashboard
Publication: 6th September 2022